تغييرات ژنتيكي و اپي ژنتيكي سوماتيكي شايع درسرطان پروستات
اين تغييرات را در سه گروه اصلي بررسي مي كتيم.
گروه اول: ژن هاي سركوبگر تومور Tumour-Suppressor genes
ژنهاي طبيعي هستند كه در تنظيم رشد سلولي دخالت دارند.بر خلاف فرآوردههاي پروتوانكوژن كه محرك رشد سلولي مي باشند، خانواده ژنهاي مهار كننده تومور معمولا از رشد غير طبيعي و ترانسفورماسيون بدخيمي جلوگيري مي كنند. وفقط در صورت از بين رفتن عملكرد هر دوآلل ژني، بدخيمي شكل مي گيرد. به عبارت ديگر بر خلاف جهش هاي پروتوانكوژن ها كه بازتاب بارزي دارند، موتاسيون هاي ژنهاي سركوبگر تومور، به شكل نهفته عمل مي كنند.
1-CDKN1B ، در جايگاه 12p 13.1-p12قرار دارد.
مهار كننده p27كيناز وابسته سيكلين را رمز گذاري مي كند. در مراحل اوليه تومور، بطور شايع فاقد يك آلل مي باشد.

2-NKX3.1 ، در جايگاه 8p21.2مي باشد.
پروتئين هومئوباكس محدود كننده پروستاتي، كه رشد سلول هاي اپي تليالي پروستات را متوقف مي كند را، رمز گذاري مي كند. در مراحل ابتدايي تومور، يك آلل آن تهي مي باشد.بيان اين ژن علاوه بر سلولهاي لومينال پروستات، دربيضه ودرسلولهاي منفردي از حالب وغدد موكوسي پري برونشيال، مشاهده شده است. در مراحل ابتدايي بيماري نسبت به شرايط طبيعي، تا 67% ازميزان بيان اين ژن، كاهش مي آبد.
توضيح، هومئوباكس يك دسته از ژنهاي دخيل در مراحل رشد و نموجنيني هستند. تمامي ژنهاي مزبور ناحيه اي دارند كه، رمز گذار يك حوزه 60اسيد آمينه اي متصل شونده به DNAاست. تجلي اين ژنها در اوايل مرحله گاسترولا آغازمي شود و تا اواسط دوران بارداري، در قطعات بافتي ادامه مي آبد.
3-PTEN ، در جايگاه 10q23.31واقع است.
اين ژن، هومولوگ فسفاتاز و تنسين كه، پروليفراسيون سلولي را متوقف كرده و آپوپتوز را القا مي كند را، به رمز در مي آورد.در مراحل اوليه تومور غالبا يك آلل آن وجود ندارد. بعلاوه در مراحل ابتدايي و بسياري از ضايعات متاستاتيك، جهش هايي در اين ژن مشاهده شده است.
4-TP53 ، درمكان 17p13.1قرار دارد.

داراي عملكرد متنوعي است كه عبارتند از:
الف، در پاسخ به آسيب DNA، سيكل سلولي را متوقف مي كند.
ب، در برابر اختلال در عملكرد تلومر، فرآيند پير شدن سلول را تسريع كرده و آپوپتوز را القا مي كند.
ج، درمراحل اوليه تومور، جهش دراين ژن شايع نيست ، ولي در 50% از تومورهاي مقاوم به درمان هورموني، موتاسيون هايي بوقوع مي پيوندد.
5-ATBF1،در جايگاه 16q22قرار داشته وتنظيم گر سيكل سلولي را به رمز درمي آورد.

درخلال سرطان پروستات، اين ژن سركوبگر توموري دستخوش missense mutations- نوعي ازجهش درdnaكه درپي آن يك باز نوكلئوتيدي با يك باز ديگر تعويض شده و اين امر باعث تغيير رمز اختصاصي يك اسيد آمينه با رمز اسيد آمينه ديگر شده ودر نتيجه يك پلي پپتيد غيرطبيعي توليد مي شود- deletionsو.... مي گردد.
6-KLF6در مكان 10p15قرار دارد.
جهش هاي نقطه اي وكاهش بيان پروتئين klf6دراقليتي از سرطان هاي پروستات با گريد بالا مشاهده شده است.
گروه دوم: انكوژن ها Oncogenes
ٱنکوژنها یا ژنهای تومورزا ژنهای تغییر یافتهای هستند که در حالت عادی پروتئینهایی را، که در کنترل رشد و تکثیر سلولها نقش دارند، بیان میکنند. این ژنها در حالت عادی پروتوانکوژن نامیده میشوند. ولی در صورت بروز جهش در پروتوانکوژنها، آنها به انکوژنها تبدیل میشوند. انکوژنها باعث بروز سرطان میشوند. جهشهایی که پروتوانکوژنها را به انکوژنها تبدیل میکنند، اغلب باعث بیان بیش از حد فاکتورهای کنترل كننده، افزایش تعداد ژنهای کد کننده آنها و یا تغییر عوامل کنترل كننده بصورتیکه فعالیت فاکتورها، افزایش یابد و یا نیمه عمر آنها در سلول زیاد شود، میگردد. به واسطه جهش در پروموتر پروتوانکوژنها آنها به انکوژنهاي فعال تبدیل شده و بیان آنها زیاد شده، تکثیر سلولها افزایش یافته و تومور ایجاد میشود.
1-انكوژن MYC، كه در جايگاه 8q 24قرار دارد.

يك عامل رونويسي است كه، بسياري از ژنهاي مسئول پروليفراسيون سلولي، فرآيند پيري، آپوپتوزيس و متابليسم سلولي را، تحت نظارت و تنظيم خود قرار مي دهد. بيان بيش از حد اين انكوژن قادر است بطور مستقيم سلول را ترانسفورمه نمايد.در تمام مراحل بيماري سرطان پروستات مقدار mRNAبطور شايع افزايش مي آبد، كه مكانيسم آن معلوم نيست.بطور شايع، ودرمرحله پيشرفته بيماري، قدري آمپليفيكاسيون لوكوس MYCشكل مي گيرد.
2-انكوژن ERG، در مكان 21q22.3قرار دارد.

انكوژن جديدي كه، براي سرطان پروستات پيشنهاد شده است. اين يك Fusion Proteinمحسوب شده و با بخش 5’ژن تنظيم كننده آندروژني TMPRSS22در مي آميزد. تحولي كه در 50% از بيماران مبتلا به سرطان لوكاليزه پروستات مشاهده مي شود.
3-انكوژن هاي ETV1-4، اين گروه درجايگاههاي 7p21.3، 19q13.12، 1q21,-q23و17q21,31قرار دارند.
اين گروه ، انكوژنها نيز مانند ERGبه بخش 5’ژن تنظيم كننده آندروژني TMPRSS22متصل مي شوند ومحصول جديدي را شكل مي دهند.در واقع عوامل رونويسي ETS- likeرا به رمز درمي آورند.
دو گروه فوق، بعنوان fusion geneتلقي مي گردند، يعني ژني كه شامل تواليهاي رمزگذار يك پروتئين از ژنهاي مختلف باشد، بدين شكل كه تواليهاي رمزگذار از دو يا چند ژن متفاوت به يكديگر متصل مي شوند. اين حالت معمولا در پي يك crossing over نابرابر ويا جابجايي كروموزمي ايجاد مي شود.چنين ژنهايي غالبا فاقد محصول پروتئيني فعال بوده ويا رمزگذار يك پروتئين غيرطبيعي مي باشند.
4-انكوژن AR، در جايگاهXq 11-12قرار دارد.
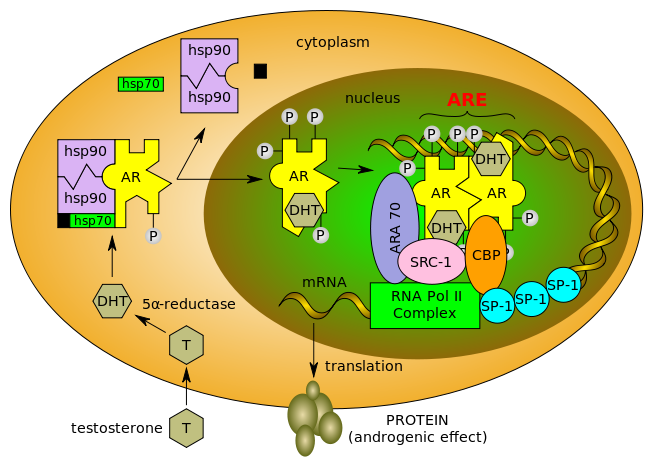
اين ژن گيرنده آندروژني را رمزگذاري مي كند.تغييرات موجود در AR signalingدرسطوح متنوعي بوقوع مي پيوندد، كه بالقوه در شكل گيري و پيشرفت سرطان پروستات، موثر مي باشد:
الف، تغييراتي درغلظت ليگاند درون سلول توموري
ب، افزايش بيان پروتئين AR
ج، جهش هايي كه منجر به تغييرات ساختماني وعملكردي مي شود
د، تغييراتي در ملكول هاي كورگولاتور مانند ARA54و ARA70
ه، ايجاد عواملي كه باعث فعال شدن ليگاند هاي مستقل از گيرنده مي شوند.
5-تلومرازTelomerase
يك آنزيم رونويسي معكوس- Reverse Transcriptase- است كه باعث سنتز تواليهاي تلومري درانتهاي كروموزوم شده و سبب ناميرايي سلولي مي گردد. در اكثر انواع سرطان پروستات ، فعاليت اين آنزيم به چشم مي خورد كه ممكن است ازطريق فعاليت ژنMYCباشد.
توضيح اينكه، انتهاي كروموزوم را در موجودات پيچيده، تلومر مي گويند. تلومرها داراي توالي نوكلئوتيدي ويژه اي هستند كه همانند سازي DNAدو رشته اي را تسهيل مي كند. تلومرها ي كروموزومهاي انساني ازنسخه هاي متوالي ازTTAGGGتشكيل يافته اند.
گروه سوم، ژنهاي Caretaker
هرگونه تغييري در ژنوم، پروليفراسيون سلولي وناميرايي آن را فراهم مي كند. بدين لحاظ در بدن ژنهايي وجود دارند ، تحت عنوانCaretaker genesكه، سبب تثبيت ژنومي در بدن مي شوند. اساسا جهشهاي ايجاد شده در اين ژنها مي تواند به بي ثباتي ژنوميك منجر شده وترانسفورماسيون سلولي را فراهم آورد.
بي ثباتي ژنوميكي بدو گروه تقسيم مي شود:
الف، بي ثباتي جهشي، كه برخواسته از تغييرات ايجاد شده درتوالي نوكلئوتيدي DNAمي باشد.
ب، بي ثباتي كروموزومي، كه ناشي از نوترتيبي ناصحيح كروموزومي است.
گروه ديگري از اين ژنها، Gatekeeperهستند، كه فرآوردههاي ژني را رمزگذاري مي كنند. بدين ترتيب از رشد بالقوه سلولهاي متمايل به سرطاني شدن ممانعت كرده وبا جلوگيري از هرگونه جهشي، مانع ازپروليفراسيون سلولي مي شوند.
گروه سوم اين ژنها، Landscaperهستند، كه فرآورده هايي را به رمز در مي آورند، كه درصورت جهش يافتن مي توانند زمينه رشد نئوپلاستيك را بخصوص از طريق حمايتي كه از جانب محيط استرومايي بد ست مي آورند، فراهم آورده وسبب پروليفراسيون لجام گسيخته سلولي شوند.
ژن بعدي، GSTP1است كه، درجايگاه 11q13قرار دارد.

اين ژن، آنزيم كاتاليز كننده گلوتاتيون احيا شده به سوبستراهاي الكتروفيليك را رمز گذاري مي كند. درواقع عملكرد آن خنثي سازي عوامل سرطان زا در بدن مي باشد. متاسفانه در بيشتر از90% ازسرطان ها، اين ژن بواسطه هيپرمتيلاسيوني كه در cpg islandواقع در upstream regulatory regionبوقوع مي پيوندد، غيرفعال مي گردد.
موارد متفرقه:
1-TP 27، اين ژن متعلق به خانواده ، CIP/KIP familyمي باشد كه پيشروي سيكل سلولي را از مرحله G1تاSرا تنظيم مي كند.در 50% از بيماران مبتلا به بيماري متاستاتيك فقدان هتروزيگوسيتي TP27 ودرضمن ارتباط فقدان بيان اين ژن با افزايش ميزان biochemical recurrenceنيز گزارش، شده است.
2-Prostatic specific membrane antigeneيا PSMA
يك گليكو پروتئين ترانس مامبران مي باشد كه نوسط اپي تليوم سرطان پروستات، بيان مي شود. در شرايطي مانند، درمان محروميت از آندروژن وبيماري مقاوم به درمان هورموني، افزايش بيان psmaمشاهده مي گردد.
3-Vascular Endothelial Growth FactorياVEGF

مدياتور مهم رگ سازي توموري محسوب شده ودر اكثر سرطانهاي پروستات بيان آن افزايش مي آبد. خاطرنشان مي كنم كه VEGFتوسط آندروژنها تنظيم مي شود. افزايش بيان آن با پيشروي بيماري و ميزان بقا ارتباط مستقيم دارد.ماركرهاي رگ سازي درسرطان پروستات عبارتند از، vegf،matrix ،metalloproteinases،IL-8، bfgf،Endoglin،Hypoxia-inducible factor 1,Tissue factorو
Tumor-associated macrophages.
4-E- Cadherin درجايگاه 16q22.1قرار دارد.
اين ژن گليكو پروتئين ترانس مامبراني را كه اتصال بين سلولي وهم چنين پيام رساني سلولي را تسهيل مي كند، رمزگذاري مي كند.در اكثر سرطانهاي پروستات بخصوص نوع بد تمايزيافته بيان اين ژن كاهش مي آبد.بدين ترتيب سلولها براحتي از هم جدا شده وبطور موضعي گسترش يافته ويا متاستاز مي دهند.
5-Epidermal Growth Factor/Epidermal Growth Factor Receptor

مقدار EGFبطور شايع افزايش يافته، وبيان EGFRدرسلولهاي بدخيم ، بخصوص با شكل گيري بيماري مقاوم به درمان هورموني، بطور فزاينده اي افزون مي گردد.
6-Histone-Lysine N-methyltransferaseيا EZH2
اين آنزيم درانسان توسط ژن EZH2رمزگذاري مي شود.موتاسيونهاي ايجاد شده دراين ژن سبب سندرم Weaver يك اختلال مادرزادي كه با رشد سريع در دوره prenatal شكل گرفته و ظاهرخاصي به صورت و فرم اسكلتي جنين مي بخشد, مي گردد.درخلال پيشرفت سرطان پروستات، مقدار ezh2افزايش مي آبد.
REFERENCES
1-Inflammation in prostate carcinogenesis
Angelo M. De Marzo Elizabeth A. Platz Siobhan Sutcliffe Jianfeng Xu
Henrik Grِnberg , Charles G. Drake , Yasutomo Nakai , William B. Isaacs
and William G. Nelson
Nature Reviews Cancer vol.7 april 200 7
2-Campbell-Walsh Urology, Tenth Edition, Volume Three
Wein, Kavoussi, Novick, Partin and Peters Elsevier 2012
3-Drug Management of Prostate Cancer
William D.Figg,National Cancer Institute, Cindy H.Chau, National Cancer Institute,
Eric J.Small, University of California,USA Springer Science 2010
4-Carcinogenic and Anticarcinogenic Food Components
W.B. Dubowska, A.Bartoszek, D.M.Gignti 2006
5-Robbins and Cotran, Pathologic Basis of Disease
Kumar,Abbas ,Fausto and Aster 8th Edition 2009
6-Wikipedia, The Free Encyclopedia 2011
7-Prostate Cancer, Signaling Networks,Genetics,and New Treatment Strategies
R.G. Pestell MD,PhD
M.T.Nevalainen MD,PhD
Kimmel Cancer Center,Thomas Jefferson University,Philadelphia Humana Press 2008
8-Genetic Terminology A.Hajibeigi, PhD R.Radpour First Edition 1381







 بنام خداوند طراح معماها
بنام خداوند طراح معماها